
That painful foot nerve
Medicine is curious. Most findings are accidental, names confuse and it takes decades to refine the truth behind the first observations. In this hopefully easy to read article, I have offered up some background research to my lectures and book. Here is a pain that Filipio, Lewis and Thomas discovered in the 19th century.
Backdrop to our story
Consider the anatomist in Italy in 1835 looking at the foot while his somewhat deceased patient allowed him some anatomical exposure. Out pops a neuralgic ganglion so says he in his later published works. This was more curious as Filipio Civinini was a cranial anatomist. By the next decade (1846), a podiatrist had identified and written about a rare but interesting pain between the second and third toes in a few patients in his treatise. Lewis Durlacher, known as a surgeon chiropodist had treated William IV and allegedly Queen Victoria.
Moving from Europe to the USA, Thomas George Morton claimed the prize and his name has stuck. First he was a published surgeon in a medical journal and secondly his observations were much more open than Durlacher. However, Morton in 1876 published his paper and talked about the fourth toe joint – metatatarsophalangeal joint. Being used to amputation surgery in the American Civil War (1861-65) he executed cutting our the joint rather than the nerve alone.
Morton’s plantar digital neuroma
A man called Hoadley removed the nerve around 1893. Much less famous than Morton he set a trend for managing this curious but rare foot problem. Indeed rare at 88 per 100,000 in females and 50 per 100,000 in males according to data taken from a large database by Latinovic (2006). Morton’s neuroma also called a plantar digital neuroma (PDN) is far more common than Durlacher’s second-third toe neuroma.
Anatomical variation
There are two reasons for it being painful around the 3-4th toes. There is a branch between two nerves that can become compressed (Diagram Govsa). That compression affects the blood supply to the nerve and the nerve swells and then becomes inflamed and produces scarring (fibrous tissue). This affects its efficiency to conduct electric signals which then become abnormal.
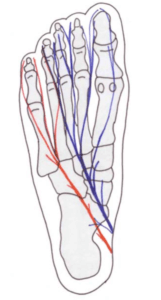
Figen Govsa 2005 anatomy study of connecting nerve branches showed 20% affected the 3-4th toes while 72% had no connection.
Podiatrist turned patient
The toe becomes numb, the small muscles start cramping, the foot becomes painful and the sensations make the brain thinks there is a stone in the shoe. Now we know ladies suffer most and we know ladies are hosts to footwear fashion, but so is this author. Well, not quite fashion but one shoe that did for me. I had a neuroma because I had the symptoms, localised tenderness was building but orthoses kept me comfortable. This went on for over 4 years and all was fine until I decided to start up cycling seriously. I bought some shoes and started cycling through the winter. Pain, numbness and shooting shocks (paraesthesia) brought me to a realisation the shoes designed to lock into the pedals of my bike were the root cause. How can this be? I’m not female by any definition.
I headed off to see my radiologist friend and we undertook an ultrasound and there it was. A steroid injection did nothing and so I was now confronted with seeing another colleague who operated in 2016. It is now 2021.
I have written the book covering my journey and lectured nationally at a Sports conferences and several smaller meetings. Next week (May 12th I am at the NEC and meeting another national meeting of health colleagues). Five more articles later I decided to write this blog for ConsultingFootPain – only this time it is for patients. I wrote an information sheet for those embarking on surgery but like most fact sheets it is only a brief summary. Morton’s neuroma is a painful condition – information sheet. This was a fact sheet I used for patients and it is dated (2018).
The concept of getting the best from fact sheets is important as much as patient articles.

ultrasound is the main method of checking the presence of a neuroma
What is it?
A small nerve (MN) is trapped between the bones called metatarsals and sends electric shock and pain signals into the toes. It can affect one foot or both feet, or it can affect more than one set of toes.
How do we diagnose this condition?
squeeze test is about 41% sensitive in the presence of a neuroma
What we now know
Nerves can recover but often start off because there is local inflammation. The symptoms of what we call neuritis can shoot back up the foot, are often short lived and occur when the foot is compressed initially. Most of the population consult someone between the ages of 40-60. However, there are some who experience the condition as early as 20-30. If caught young then recover can be encouraging.
In 1995 Gordon Bennett looked at 115 patients and followed them for 2 years. Thirty-nine percent did well with insoles and footwear alterations. In other words altered their footwear. Baransel Saygi (2019) found that if steroid was added to using insoles the benefit increased over 1 year from 11% to 82%. This would only work because the shoes that are used to accommodate orthoses have to be better than shoes previously used by the patient.
Steroid injections
Steroid injections have been used extensively and more has been written about the follow up of large patient groups than any other form of injection. Taken collectively, improvement can be less than 50%. Most follow ups have not exceeded the 2 year mark. In a 2017 study by Grice (2017) the immediate results shot up to 87% but then dropped at 2 years to 31%.
Clinical evidence
Two excellent papers have been produced, one by Daoud Makki 2012 and another by Young Park 2018. Using ultrasound to measure the size of the neuroma, they found that those smaller than 6mm in size respond better than when larger. The normal size of a nerve should be well under 3mm. The size increases because of scar tissue, swelling of the surrounding soft tissues which remain engorged with inflammation.
Once the nerve has expanded, Sunderland 1953, considered the nerve beyond repair. To make one feel a little more relaxed, some nerve do grow as was found under the more detailed MRI scanning process. Bencardino (2000) identified 33% of her scan had larger nerves, some measuring 10mm. The scientific community have still not answered all of the fundamental questions but clinicians have tried new methods.
Imaging the nerve
The value that imaging – ultrasound and MRI brings relates to refining the diagnosis so fewer misdiagnoses are made. The size can be measured but both methods are not as precise than measuring the damaged nerve under a microscope.
Alternative methods
Radio-frequency treatment under local anaesthetic has gained popularity and even the Government agency NICE have approved this treatment with caution. Freezing (cryotherapy) appears to have a place and the results and risks equate to surgery. Capsaicin (chilli powder) has been used but the study was too small. Hyaluronic acid (think glucosamine) has been used, but again only one useful study, but this does not mean more research. Alcohol has gained more research recently. This is usually diluted and takes the form of ethanol or phenol. Pabinger (2020) believed that alcohol could shrink the size of the neuroma in some cases. The longest study I have come across was from Elena Samaila using phenol in 125 patients and followed her group for up to 8 years.
Many of the studies conducted have been badly designed and if limited scientific value because patients are not invited into a study as they should be with controls. Many studies look backwards and so controls cannot be applied. For example, many clinicians used steroid injections as well as other methods. Mixing treatment removes the purity of any study.
Di Caprio (2018) reviewed many papers amongst a number of researchers and agreed with Gordon Bennett on making sure patients first had conservative treatment. However it is recognised that unless you can spot symptoms early many of the treatments suggested fail.
 You will notice that pain medicines have not been discussed and are rather more the domain of the GP who, and forgive my cynicism, apply pain medicine for feet as a holding mechanism. Sadly this is old fashioned, it is unrefined medicine and is part of the problem seen in the UK’s collapsing NHS system because if waiting times. So many conditions require earlier tests (imaging) and treatment to prevent deterioration. Without early intervention conditions such as neuroma become less manageable and end up with surgery which as Di Caprio points out is at best 85% successful.
You will notice that pain medicines have not been discussed and are rather more the domain of the GP who, and forgive my cynicism, apply pain medicine for feet as a holding mechanism. Sadly this is old fashioned, it is unrefined medicine and is part of the problem seen in the UK’s collapsing NHS system because if waiting times. So many conditions require earlier tests (imaging) and treatment to prevent deterioration. Without early intervention conditions such as neuroma become less manageable and end up with surgery which as Di Caprio points out is at best 85% successful.
Stump neuroma
A stump neuroma from Morton’s neuroma surgery occurs in the foot resulting from the surgery which removed the Morton’s neuroma. It is a nerve disorder, which leads to extreme irritation and swelling in foot nerves and can be extremely painful. During the surgery, the nerve is cut and this can lead to a small growth from the end of the nerve – a ball of nervous tissue, which is known as a Morton’s stump neuroma. It is also called a “recurrent neuroma” as it is a reoccurrence of the initial Morton’s neuroma and it may also be referred to as a “failed Morton’s neuroma surgery”. Morton’s stump neuroma can be a source of great pain for patients. Any type of mild or low pressure exerted on Morton’s stump neuroma can cause pain, which even includes brushing of clothes against the affected site. (Pearl, Janet MD, USA)
And so what happened to my foot? Well I did well for 18 months but after surgery symptoms actually reoccured. What was around 85% successful dropped to 70% as time progressed. I have been at 55-60% success and had an alcohol injection, now at 1 month duration. I have fallen back to my orthoses and get good days.
The ethanol injection was given under local anaesthetic and for 48 hours the pain was intense and at one point required ibuprofen. I would place my foot at 60% still and my decision for surgery or revision surgery is on hold. Dr Janet Pearl has a good site on the subject of Morton’s Neuroma and I believe produces some good material. The site was accessed 27/4/22.
What’s the final advice?
In summary the bottom line is be wise. If you have pain that affects around or between toes seek advice. An insole or orthosis is still a valid method. Avoid multiple injections of steroid as someone is making money if one fails. Two maybe, more – then seek more expertise. This site cannot direct you to anyone specifically but in the UK a podiatric surgeon FRCPodS or a specialise orthopaedic foot surgeon FRCS are best. In the USA go to a DPM podiatrist or a foot orthopedist. The reason for seeing this specialists is because they can provide the full panoply of investigations and have good hospital connections.
If seeing a UK GP ask to see a foot specialist – this is someone both qualified and trained both in medicine, orthopaedics and podiatry foot health. In the UK all podiatrists are licensed to practice through a Government recognised register called the Health and Care Professions Council.
You can read my surgical journey in my book Podiatrist Turned Patient: My own journey
available on Amazon and you can read the reviews on CFP
Thanks for reading about ‘Morton’s Nerve Pain‘ by David R Tollafield

Sign-up for here my regular FREE newsfeed
Published by Busypencilcase Communications. Est. 2015 for ConsultingFootPain
![]()
Recent Comments