
Ankle Fracture v Ankle Sprains

Dr Paul Stepanczuk DPM
This article covers ankle fracture v ankle sprains and comes from the pen (or keyboard) of my North American colleague Dr Paul Stepanczuk DPM. I first me Paul in Autumn 1981 and we often share notes, get together, or we did before Covid and flight restrictions. We have attended clinics and theatre together during our long and healthy period of liaison. Paul wanted to share his own experience in the diagnosis and approach to minor trauma of the ankle. While a number of podiatrists are involved with trauma centres in the USA, many more foot specialists manage lower grade injuries which contribute to chronic pain in the foot and ankle. In the UK ankle management tends to fall to orthopaedics but British podiatry is forever expanding its role, none moreso than in sports podiatry.
Paul discusses a case from practice
This was a lesson learned quite early on in my career. X-rays may not always be necessary, but evaluating the process of an injury and a thorough anatomic exam always are important. This patient, in his twenties, was bothered by a “painful ankle” for several years and injured during a family picnic. He was treated by a GP, without any x-rays being taken and diagnosed as “only an ankle sprain.” Consequently there was rudimentary treatment without follow-up.

Standard form may use the Ottawa Rules for ruling out a fracture click to see film 1.59′
Symptoms persisted at the original site. Discomfort affected his gait, so perhaps this new podiatrist in town could have a look at it and see if any further treatment could help.
Standard ankle examination
A standard ankle exam revealed no lateral ankle pain but discomfort existed over the anterior calcaneal process. An oblique x-ray revealed a slightly displaced fracture with non-union and a distal fragment over 1/4″ (0.25 cm) long. Closer inspection showed the fracture edges were rather rounded and well-defined indicating that no further healing was likely. The fragment was surgically removed and relief eventually achieved.
Examining this area of the foot became standard for me from then on with any rotational injury of the ankle or rearfoot, and a few tiny fractures were noted over the years. During my 40 year career, patients similar to this came in at various ages and at various time frames. It seemed, back then, that the so-called common ankle sprain was the most under-treated injury known to mankind, and the number of post-traumatic cases of instability and arthrosis were significant. Over time I developed a routine (protocol) for ankle injuries that, I think, stood well for all concerned.
The patient was asked to point with one finger as exactly as possible where the pain seemed to arise. The exam developed from there. The foot doctor needs to examine each anatomical structure individually (in that area) commonly known to be subject to injury and if the structure is bone then definitely an x-ray is indicated. Obviously this initial sequence may need modification as the patient may not be at all able to bend over to point. The swelling from a fresh injury may hide the usual landmarks. The pain from pressing anywhere may prohibit a good exam. Perhaps there may be a case where something definitive must be done right away, but I never came across that circumstance, so, if nothing else could be accomplished, a posterior splint and gentle wrapping supporting the foot and ankle comfortably could be applied.
Instructions should include:
- eliminating all unnecessary weight bearing.
- elevation of the injured part at a high enough level such as above the hip line
- Correct method of applying ice without damaging the skin
- length of time to apply ice 20 minutes with a break of 2 hours between
- (shorter application times and longer rest periods if older and skin is fragile
- observing follow-up 2-4 days later
Next stage
Once the swelling and pain have decreased, enough to complete the basic, thorough exam, further planning can begin. You can then discuss the findings with the patient and why necessary steps must be taken.
This case generally illustrates how a problem may be disguised as something less significant. A fracture may easily be overlooked unless specific steps are taken and so may be left under treated. Untreated fractures can exacerbate problems in the future. When it comes to sprains is considered all areas to include the ankle proper, the hind foot and subtalar joint and the talo-navicular joint ligaments and tendons need to be individually evaluated. Again introduce an x-ray if bone involvement is suspected. When it comes to the lateral ligaments – antero talo fibular and calcanei-fibular ligaments, examination under local anaesthetic (common personal block) or general anaesthetic may be required as guarding will limit the value of a decision that is intended to lead to foot and ankle surgery. MRI is particularly valuable.
Anterior process fracture
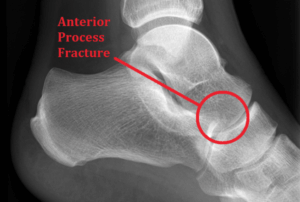
The circle shows a chip fracture. Citation – photo from https://ankleandfootcentre.com.au accessed 3/2/21
In the few other instances of anterior process fracture relief was gained by applying a below-knee cast for 4 weeks with the ankle neutral after initial swelling had subsided.
Cases of other acute ankle injuries that I treated ran the gamut from very simple sprains to single malleolar fractures. Treating these injuries morphed over the years secondary to treatment technology advancement. Over time better ankle splint designs have revolutionised patient care. Learning what seemed to work best for my patients who came to my office complaining of persistent problems was an important part of learning. It soon became clear that a certain amount of rigid stability coupled with a certain amount of flexibility and for a sufficient length of time would produce the best results. Elastic (ACE – Trade Mark name) bandages seemed to not provide enough stability, although the occasional patient would swear by them.
Ankle braces
 Removable and reuseable stirrup-type ankle braces were being developed. These days there are a number of iterations of this basic design, but the concept remains the same: medial to lateral stability is achieved while ankle dorsiflexion-plantarflexion is allowed. It also became clear that length of time these were used was also important. Those that discontinued them prior to full relief tended to have the persistent sequellae of pain and arthrosis. The illustration shows a women managing to get around a supermarket shop aided by a typical ankle brace preventing frontal plane movement. Sagital plane movement can still occur and the shopping trolley helps. This would be used once the main swelling and pain had subsided and the diagnosis had been assessed.
Removable and reuseable stirrup-type ankle braces were being developed. These days there are a number of iterations of this basic design, but the concept remains the same: medial to lateral stability is achieved while ankle dorsiflexion-plantarflexion is allowed. It also became clear that length of time these were used was also important. Those that discontinued them prior to full relief tended to have the persistent sequellae of pain and arthrosis. The illustration shows a women managing to get around a supermarket shop aided by a typical ankle brace preventing frontal plane movement. Sagital plane movement can still occur and the shopping trolley helps. This would be used once the main swelling and pain had subsided and the diagnosis had been assessed.
The importance of maintaining support
So I incorporated those findings into the treatment discussion advising patients that we usually immobilized a basic bone fracture for 4 weeks in the average adult, and that since blood supply to a ligament was less than bone, it was reasonable to think ligaments needed to be splinted for at least that long or longer. Failing to do this risked some amount of excess movement (wobble) where the ligament was supposed to hold 2 bones at a certain anatomical distance. This seemed to lead to chronic ankle sprains preceded by the phrase “doctor every time I step off a curb or step off a bus I sprain my ankle” or arthrosis/arthritis of the ankle joint itself. Sometimes I could still treat these patients with ankle splintage on an as-needed basis. Sometimes I had to refer them to other practitioners who performed arthroscopy or joint replacement. And all these situations referred back to taking a thorough history of the injury, a thorough proper examination of the proper site, and initiation of treatment of sufficient length of time.
More information
More articles on ankles can be found on this ConsultingFootpain site to assist patients and help them understand some of the concerns mentioned in this article.
Ankle Sprains and Strains
Acute and Chronic Pain
The Second Ankle Joint
Treating Simple Ankle Sprains
The Third Ankle Joint
Chronicity and the Lateral Ankle Sprain (Professional Talk)
Additional resources
from one of my trusty sources: footeducation.com provided more information about ankle instability. More on ankle fractures.
Thanks for reading ‘Ankle fracture v ankle sprain’ by Dr Paul Stepanczuk DPM
Published by Busypencilcase Reflective Communications Est. 2015
![]()
 why not sign-up to regular newsfeed articles from ConsultingFootPain
why not sign-up to regular newsfeed articles from ConsultingFootPain
Published 9 March 2021

Recent Comments