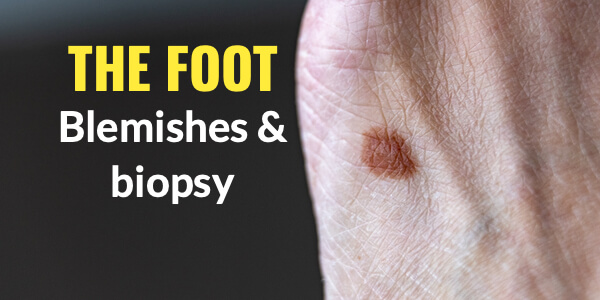
Sampling skin lesions on the foot
Quick reference article with links
As part of the field of podiatry is deciding to expand its skill set ConsultingFootPain wanted to produce an introductory article covering the objective of biopsy in the foot. You can read more about the latest course from the Royal College of Podiatry after CFP interviewed the organisers and delegates last year.

is available within this article and contains sensitive material
Biopsy
A biopsy is a medical procedure that involves taking a small sample of body tissue so it can be examined under a microscope (NHS). The important part is to realise that there are several ways a sample is taken. Most podiatrists in the UK do not undertake deeper surgery than the skin, except podiatric surgeons licensed and registered with the HCPC. The skin, being both visible and superficial to other structures often shows changes that are difficult to decide whether there is a change that leads to concern. The key areas that are easily missed include under the nail or between the toes. As we age, reaching the foot and seeing the foot can be challenging by the limitations of inflexibility. The sole can hide blemishes, while swellings can at least be felt by hand.
The good news is that the foot while having many blemishes, does not present life-changing problems as common as we might believe. The last thing any responsible professional wants is a stampede of pointless referrals wasting time on the one hand and yet not dismissing worry on the other. However, the skin often shows more cancer than deeper parts such as bone and joints or muscles. Cancer does not have to be life-threatening and some cancers are slow to arrive and can be managed.
The key signs of abnormal changes include an area that changes colour, bleeds, itches, changes shape or alterations to the surrounding border. We call any change from normality a LESION. Any change in a lesion should be photographed, dated and followed carefully. The indications, should they arise as stated suggest an early consultation is needed. Phone the GP practice and tell the reception staff that you have an area that has changed on the foot and would like to see someone. Today 111 is a direct helpline to the NHS (UK) and someone will guide you if you cannot see a GP. Podiatrists can guide you as well and many now have introduced special diagnostic tests such as dermoscopy to improve the diagnosis and classify whether a referral or a biopsy is required.

C/O Dr Ivan Bristow The Foot Expert (Foot dermatology)
We do not want to cut into the skin unless absolutely necessary and then to confirm our suspicions and provide treatment. Treatment can range from heat or cold, laser and cryotherapy, or surgery.
Surgical biopsy
There are several techniques available to the surgeon. We can shave the top to acquire a sample or we can punch a section out using a small punch. The last technique is an excisional biopsy, often used as part of treatment. Shave, punch and excisional biopsy are different techniques. The biopsy is designed as a diagnostic method of testing for abnormal skin cells. Sometimes needles are used and the method is called a needle biopsy, but, for the most part, we use needles to draw fluid for sampling for infection and gouty crystals seen in joints.
Preparation
Local anaesthetic is used in the main for these outpatient-based procedures. This means you can go home after the procedure has been completed. Pain medication is recommended if the area is likely to be sore or more than one sample has been used. The cells are placed in a pot and sent off to the laboratory to be viewed and reported on. The sample is carefully handled and then slices are cut so it fits under a microscope on a glass slide. Simple samples are returned usually within a week although it depends on the urgency stated by the clinician.
Shave biopsy is often used for lesions that stick up and have thin stalks. They are not ideal for lesions that involve deeper structures. As a podiatric surgeon, I would prefer to remove the whole lesion taking some healthy tissue with the sample. One of the things I learned when training was that my consultant pathologists would scribble all over the report that an insufficient sample was taken. This is embarrassing for the clinician and of course, the patient may have to come back for a repeat procedure. The reason that pathologists would rant was that they need healthy side tissue to make a reasoned comparison.

standard biopsy sampler 4mm + in diameter
A punch biopsy is generally better for flat lesions that have depth. These are valuable because the site heals quickly. The sampling technique is fast and can reach down to the bone to ensure the pathway is free of abnormal cells. The diameter varies with these punch biopsies from 4 mm upwards. I found I could punch through a nail so as not to remove the nail plate which is better for the patient. One of the problems with punches is that if the diameter is small you may not capture the edge where healthy tissue exists invoking an angry scribble on the report! Smaller punches can prove difficult in retrieving the sample. Sutures are less likely than with excisional biopsy but of course, as the diameter widens closure may require a suture.

The following link is useful and offers some more material. Click here. The YouTube film may be useful for students and those with stronger constitutions. Click here for video
Excisional biopsy is the standard for lesions in general for two reasons. It provides visual depth and the surgeon can assess the changes in tissue offering a high suspicion of concern or not. The lesion can be excised to offer good sampling of normal tissue. The closure is made with steristrips (tapes) or sutures. It is in effect a surgical procedure and must be carried out to the same standards as any surgery. The 35 sec video helps the uninitiated to understand this technique
Summary
Three techniques are shown, each has a specific indication and benefit for sampling lesions of the skin with reference to the foot.
For the clinician, planning is important and larger areas of excision are best performed in a dedicated theatre environment. Too much skin removed can make closing the gap difficult or the gap may have to be left open and packed. The use of dermoscopy has reduced the immediate need for surgical biopsy where the lesion may be unclear to diagnosis.
Remember most lesions are harmless and take time to develop problems. However, if the site is painful, itching, changes colour, bleeds or discharges and the border has lost shape, then it is important to obtain a medical opinion early.
The foot may be hidden but can be exposed to the sun, the skin may burn when on the beach or outside in the open. Injuries that may appear to partly heal can turn nasty and infections, if left, can also alter the skin cells and become malignat.
Be SAFE, SEEK an opinion, STAY alert

Sign-up for here my regular FREE newsfeed
Thanks for reading ‘Biopsy in the foot’ a short introduction to the benefits of biopsy in the foot by David R Tollafield
Published by Busypencilcase Communications Est. 2015 for ConsultingFootpain
![]()
Recent Comments