The rationale behind the orthosis in foot care today
Do we just accept what a foot orthosis does without any fundamental knowledge behind defining a product sold by a wide range of outlets – often without any sense of professional assessment? This information will allow you to understand the broader world of orthoses and orthotic management with some caveats. I defined orthosis as a quick reference article and wanted to expand a little, partly as it charts some of the history for those who seek more science behind the subject of orthoses.
The subject of orthoses must be aligned to biomechanics associated with modern-day musculoskeletal (MSK) health for podiatrists. It is important that patients know why they are guided towards this type of product and the importance of the terms used.
‘Ortho-‘ is the prefix to many words like ‘orthopaedics’ – straightening children if we crudely translate this term. Many terms have been used to imply the same type of device for feet – insoles and appliances being the leading alternatives. A prosthetic device is excluded, but feet sometimes require a combined product that has an orthotic effect. From a thin leather board to thermoplastics, podiatrists learned how to manufacture material to a commercial level until health and safety made isolated manufacture unprofitable. Orthotic laboratories grew to provide aesthetically more acceptable orthoses based around a clinical prescription.
 How do we cover 100 years of development in understanding the foot without writing a book? I wanted to embrace an understanding of orthoses with pressure and force measurement associated with modern orthotic prescription. Having made a career from the science and provision of orthoses for patients, I am equally aware that there is a parallel industry that can mislead patients. Podiatrists care about ambiguity and inappropriate sales pitches. This article is intended to offer an introduction to both the student and the lay reader. The subject of biomechanics is complex and not to be confused with a pure assessment of the human framework. My goal was to keep some of the technical detail to a minimum.
How do we cover 100 years of development in understanding the foot without writing a book? I wanted to embrace an understanding of orthoses with pressure and force measurement associated with modern orthotic prescription. Having made a career from the science and provision of orthoses for patients, I am equally aware that there is a parallel industry that can mislead patients. Podiatrists care about ambiguity and inappropriate sales pitches. This article is intended to offer an introduction to both the student and the lay reader. The subject of biomechanics is complex and not to be confused with a pure assessment of the human framework. My goal was to keep some of the technical detail to a minimum.
Background history
In Australia, podiatrist Philip Vasyli started to change the landscape of commercial orthotic provision. After a tragic death, he has left a living product available from many outlets sold directly to the public. In the meantime, carbon fibre and similar products were produced, often from computerised patterns from scans of feet as part of a prescription service. As a result, the accuracy of the orthosis was far more precise than the older insole. Today’s products and how they were developed however emanated from the 19th and 20th centuries. Shapes were drawn around the foot or from the inside of the shoe before placing foams between the lower material (leatherboard) and upper material leather. As plastics became refined, they replaced leather and rubber materials. Most people will have come across the steel arch plates with their rivets, promoted by Scholl’s, an international commercial firm selling over the counter foot health products. These thin metal orthoses, with some made from stiff leather, were mass-produced but failed to cater intimately for the heel and variety of sole shapes and arch heights. The steel plate was strong and lasted without the need for replacements. However, the heel was flat and to the modern podiatrist, this appeared to offer ‘no control’ to the patient. Vasyli’s orthoses had contoured heels and could be adjusted with the application of heat as well as produced in different densities.

Top left: traditional commercial soft insole with arch raise. Top right: customised insole made to prescription c.1978. Bottom left: orthoses made from casted models c.1980. Bottom right: traditional customised appliance with toe/tarsal straps c.1978
In the USA, from the sixties, the earlier designs were based around a popular subject called ‘biomechanics’. This was a pseudo term but contributed to podiatric medicine degree in the USA. Much of this pseudo-science involved measurements with protractors (tractographs) and in build error ‘eyesight’ assessment which led to assumptions with a predilection for the concept of wedging. The foot orthosis (F.O.), as it was called, tried to separate itself from the older insole and appliance. A google search today will still confuse the terms.

A modern mass-produced orthosis made from light thermoplastic materials with contoured heel and full length designed following the pattern of the older insole.
There was a strong rationale behind specific foot shapes being better managed with orthoses rather than insoles because in the latter case there was no intimate relationship with the hindfoot. For example, the definition of the front of the foot being called ‘forefoot varus’ or ‘forefoot valgus’ depended on which way the foot leaned when viewed from behind the heel. The forefoot position would affect the hindfoot as much as the hindfoot could affect the midfoot and forefoot. An understanding of the co-relationship between foot joints became important when offering patients better products to help their foot pain.
Doctors of podiatry in the USA; Merton Root, William (Bill) Orien and John H Weed, made a name for themselves on the west coast of America. Across the USA, various theories arose with vociferous debate and claims. By the early eighties, the new ideas behind assessing the foot crossed over to the U.K.and the older regenerated leatherboard insole started to lose popularity, criticised for inaccuracy, lacking science and commercial value. U.K podiatrists took on board many of the theories and hypotheses that had now grown in the USA together with its expanding commercial orthotic laboratories. Alongside surgery, orthotic provision became a lucrative source of income for the profession. Initially, the laboratories were closed to professionals but then opened up as the commercial opportunities grew. Enter Vasyli, who demonstrated his commercial business prowess and kicked down the cost of a pair of orthoses. Gone were the days of grinding and manufacture for the average podiatrist who could concentrate on altering the newer materials by adhered wedges and heat guns.
Biomechanics as a true science
Sheldon Langer and Justin Wernick were two podiatrists who influenced the changes in podiatry within the U.K through the Podiatry Association and A. Paul Barcroft. They introduced technology such as the Electrodynogram (EDG), the first commercial podiatric foot pressure measurement tool using transducer technology through microcircuits (c.1979). Promoted on Britain’s popular scientific programme – Tomorrow’s World, the EDG looked as though it could overcome some of the spurious handheld measurements.
United kingdom developments
In the UK, biomechanics and human motion were studied by bioengineers and clinicians. R. Betts, Peter Cavanagh, W C Hutton, G Drabble, Sandy Nicol, David Pratt, John Foulston to name but a few British scientists had studied mechanical forces with specialised pressure sensors of which the Kistler force plate was considered the most accurate. The idea that biomechanics related to the measurement of the joints of the foot alone was criticised without the knowledge behind how the body’s skeletal tissues (bones and joints) responded to external forces and muscle-tendon influence. Marrying science with clinical conditions became the goal that all podiatrists aspired to and this influenced changes within the course syllabus in colleges which then became departments of health science within Universities.
 The EDG by now was not as sensitive or accurate for its intended purpose although it aimed to offer the clinician a diagnosis as an early type of artificial intelligence; guiding treatment. Pedobarography became another popular tool during the seventies that developed from a colour shaded impression of pressure – light = lower pressure, dark = higher pressures (shown). Black and white shades developed into colour and then measurement was introduced. The use of pressure squares or mats required patients to place their foot in the centre of the square such as the Kistler and later the pedobarography. The earlier pedobarography had a glass top on raised platforms utilising the concept of mirror reflections of a bathroom footprint – as in high arch, low arch.
The EDG by now was not as sensitive or accurate for its intended purpose although it aimed to offer the clinician a diagnosis as an early type of artificial intelligence; guiding treatment. Pedobarography became another popular tool during the seventies that developed from a colour shaded impression of pressure – light = lower pressure, dark = higher pressures (shown). Black and white shades developed into colour and then measurement was introduced. The use of pressure squares or mats required patients to place their foot in the centre of the square such as the Kistler and later the pedobarography. The earlier pedobarography had a glass top on raised platforms utilising the concept of mirror reflections of a bathroom footprint – as in high arch, low arch.
The development of the EDG had overcome the need for the patients to land on a small designated space as it had adhesive pads stuck to the foot. In-shoe and sensor pads became a better direction of travel to measure the foot in contact with the ground and this started to emerge as the front runner for clinics while the force plate mats became more popular for research departments. The whole science and technical development applied to many different professions although podiatrists naturally were heavily involved with questions like; do patients with certain problems with feet have higher pressures and different distributions of forces that caused problems such as skin changes and ulceration. Could we predict and prevent ulcers by knowing that a foot had already started to change from normal pressure distribution?
Overcoming problems
The complexity arose because different interfaces between the foot and ground could alter the pressures. Different shoe designs and material properties naturally would change these foot pressures. While scientists could produce very accurate measuring devices, measuring the direction that forces acted upon the foot offered greater challenges. A foot when contacting the ground would not just have a vertical force but a lateral force – that meant at least forces acting in two D. In fact, this was even more complicated as the foot surface rotated twisting as well. Thinking in terms of one or two dimensions provided a narrow understanding of the foot in dynamic positions. The foot had to be measured in 3D as forces arose in three directions. The questions that arose in those early days still exist today.
We can measure forces between the foot and the ground. Once the shoe is fitted to the foot these forces change as mentioned above. The shoe has material in the sole and insock (inner sole) that alter the pattern of foot force over the foot. We modify shoes and insole interfaces as part of treatment to reduce the forces causing high-pressure points.
Is it better to measure without a shoe or not?
One way of solving this takes us back to the EDG. However, sticking a dozen pads to the foot fails to account for every part of the foot in contact with the ground. When we run the heel hardly touches the ground at speed. There were also technical issues with transducers not least their life span expectancy and accuracy of multiple-use.
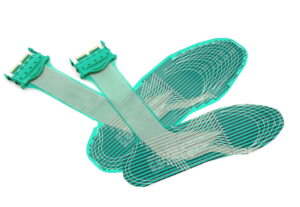
Tekscan system for measuring in-shoe pressure
Linking the in-shoe problem with the body
Adhesive transducer pads have now given way to an insole (shown) attached to wires that lead to a backpack that communicates with a computer. Tekscan is one of a number of modern systems used by clinical centres. While all this was developing, the scientists appreciated that the body above also was important and ground pressure should not be measured alone. We came back to an older science, that of kinematics and spatial changes of the body.
As injured soldiers returned from Iraq and Afghanistan, modern equipment was used to ensure new prosthetic limbs were developed to higher specifications. Gait laboratories had already developed a long time before these foreign wars were engaged. A number of centres were associated with orthopaedic or rheumatology funding within the NHS to provide better care. The centres were often run by bioengineers who interlinked the footplates or platforms to cameras that picked up reflective discs using infrared technology. The amount of information was huge coming from information about foot, leg and body movement. Many podiatry practices had implemented gym type treadmills. By using video footage of patients in slow playback, patients could see some problems when the foot contacted the ground from their rigid state to flexible positioning indicating between stable foot function to unstable foot function. Terms such as pronation and supination, denoting the abnormal side of low and high arch tendencies had been widely accepted and ‘pronation’ was on everyone’s lips and in all the sports health magazines.
Modern podiatry
Today podiatry practices incorporate some of the newest technology to show foot pressures. Most of this is carried out by the independent sector rather than the NHS. Examples such as the Ideal Home Exhibition often attract salespeople who use pressure mats to convince the lay public that they need orthoses. The sale pitch offers a free assessment often by an unqualified person who will sell the product to clinch the sale.
The graduate podiatrist understands the difference between the commercial pitch, the methods of assessment that have value and those that are invalid. We are better informed by marrying modern science with medical orthopaedics as we understand how muscles and joints work under pressure. The diseases that affect joints must be considered and the neurological variations that require testing. The loss of sensation and damage due to pressures in different directions make up many foot problems. It is doubtful that any salesperson could have any sense of understanding without a minimum of five years of study at degree level in foot health science.
Choices
We now see two distinct orthotic types on the market from these early beginnings—those available from internet sources and chemists and those prescribed by professionals. There are parallels with the sale of glasses and foot orthoses, a method Sheldon Langer used to sell orthoses to the profession in the eighties. An orthotic could facilitate the correction of a defect. By controlling a painful or unstable foot, an orthotic could be constructed on a plaster cast of the foot to have an accurate contour. The foot, once corrected, would alter the muscle balance just as the prescription lens would alter the optical muscles to improve sight. Vision is now equated to locomotion (human movement). As human movement scientists became experienced, we knew that the foot and leg were intimately controlled through the ankle bone (talus). Therefore, a foot orthosis could control the leg rotation and thus aid knee pain and hip pain. Some patients even found back pain improved as the movement was modified through the foot. The old Scholl orthosis worked on ‘jacking’ up the arch until the client could no longer tolerate the discomfort. Unfortunately, this paradigm is still a problem that a specialist must guard against because using a painful orthosis will hardly be used if it languishes in a drawer.
Should prescription orthoses be used alone?
It would be a great sales pitch to say yes, absolutely, but that would show a lack of professional ethics and probity. If you have a foot problem and considerable pain, a professional diagnosis is essential. Even medical doctors are not trained in foot health to any depth. Most G.P.s know who and when to refer on.
An over-the-counter orthosis will not harm most people. Like paracetamol (Tylenol), it is often better to try the analgesics for 24-48 hours before consulting the doctor. The soft material, if helpful, is fine, but there is no intimate foot control. The stiffer and less flexible materials can cause more problems depending on the foot type. As a podiatrist, my role was diagnostics and surgery rather than issuing orthoses. I would source inexpensive orthoses for my patients and then refer them to a specialist podiatrist.
prescription orthoses are not required for most people
Prescription orthoses are not required for most people and some lower-cost alternatives are perfectly adequate. Vasyli was a major influencer in this marketplace.
A podiatric consultation is wise for those with medical foot problems (diabetes, rheumatoid, psoriatic arthritis, compound arch pain, or deformity). High-performance athletes are best consulting a podiatrist with a sports interest as the market is broad and confusing for laypeople. For the average person with a typical intact neuromuscular system and normal bone and joint development, expensive, highly technical gait assessment laboratory work is not required. However, visually recorded gait patterns are often invaluable for charting progress and can improve muscle work. Commercial pressure platforms can identify abnormal pressures and guide altered posture but should be only used by trained professionals with appropriate qualifications. There is NO REGULATION of this sector.
An orthosis is a facility to help improve foot function alleviating pain and poor tendon and muscle function. For example, forefoot pain, often loosely called metatarsalgia, will improve because the orthosis can alter the pressure distribution. Additions to orthoses can be added but preferably with professional guidance.
A story from the past
As I completed my studies in 1978 I was invited to the nearby university in London to observe a new system of foot pressure analysis. The patient walked along a designated walkway in a narrow room and placed their foot on a square marked section. The computer that analysed the system was next door and took up as large a space as that of the gait analysis room. Today we all walk around with thin handheld computers called SMARTPHONES and TABLETS. These have more computing power than those systems that had to reside in air-conditioned rooms. I marvel at the speed of change and feel proud to have shared in such technological changes during my career as a podiatrist.
David Tollafield is a registered podiatrist and qualified from University College Hospital (London Foot Hospital) in 1978. In 1981 he travelled to the USA to study podiatric biomechanics sponsored by the Silver Jubilee and Churchill Fellowship Foundation. His first degree was in transducer studies in the foot and human locomotion at Coventry University (1990). He was awarded his Fellowship of the Royal College of Podiatry in Podiatric Medicine FRCPodM in 2012 and his surgical fellowship FRCPodS in 1986. He was Director of Curtis Orthotic Laboratory (1981-85) and senior lecturer in Podiatric Orthopaedics at the University of Northampton (1985-1994). His autobiography – “Podiatrist on a Mission”, is available from Amazon, published by Busypencilcase Communications 2021.
You can read more stories about podiatry and foot health in David’s publication available as an ebook and paperback from Amazon books

Sign-up for here my regular FREE newsfeed
Thanks for reading ‘Biomechanics and the foot orthosis’ by David R Tollafield for ConsultingFootPain
Published by Busypencilcase Communications. Est. 2015
1 March 2022
![]()
Recent Comments