
An unusual location for a corn
Extensor hallucis longus and the dorsal intractable keratoma
This case history applies to all podiatrists, including foot surgeons. It concerns a 73-year-old female who presented with a lesion over her left great toe’s extensor hallux longus tendon. Debridement and enucleation revealed a clear fluid; the tissue was not infected but appeared long-standing. Sandra was well dressed, had no medical history of concern, took no medications, and suffered no allergies. Her footwear typified a lady who cared for her appearance, like the shoe upper cut into the pronounced tendon.

Standing position demonstrating EHL overpull. Ref: Heo, Youn-Moo (2010)
Examination of her gait showed a prominent EHL; the toe retracted through the swing phase of gait and remained active for longer than ideal. The B&W image (above) shows a patient with contraction of the tendon can occur with injury as well through tendon imbalance. The first metatarsal was thus plantar flexed due to the position common to this foot type and the contracting effects around the retinaculum and extensor apparatus (illustrated). The extensor intractable dorsal keratoma (EHIDK or IDK) carries a similar difficult prognosis once established to the plantar intractable keratoma – deeply established with complex dermal invagination. Podiatric core treatment would involve three principles: footwear advice, redistribution of pressure, and altering the mechanics with an orthosis.

Case history female 73. Recalcitrant corn (intractable keratoma). The top images show the lesion before debridement. The bottom right image shows reduced crease as the operator pulls the toe to show a reduction of extensor hallucis longus overpull
Essential Podiatry
As a student, I first came across this form of IDK and applied, as directed, a tendon pad. The pad was made from felt and shaped with curved corners, bevelled to enwrap the toe after a channel had been cut through the adhesive base. It was a cardinal sin to adhere any felt (or similar) pad to a tendon so it could not move. The non-adhesive solution would be to use a foam sleeve before any siliconised gel alternatives had been created. The silicone gum and catalyst introduced in 1970 offered a newer method created from an interdigital anchor at the time. The material had to be crafted not to fill the toe box.
As a student of the time (1975-8), I thought such lesions were difficult to cure but could be helped enormously. Fast forward to 2016. Sandra had received podiatry and her podiatrist could do no more; hence she appeared on my clinic list. The surface callus was debrided but the appearance of the lesion was chronic. Pressure had caused some leakage but no sinus or obvious abscess was underlying the tissue. The chronic nature of the IDK means that padding, although it provides temporary relief, will not yield a permanent outcome unless the patient is willing to change her footwear permanently. The second problem arises from the extensor substitution, which creates a plantar flexed toe. One must balance up the patient’s willingness to have intensive treatment to offload the area, select orthoses to reduce the extensor substitution and hope there is no reoccurrence.
Judging by appearances
The key phrase “…who cared for her appearance…” is critical. Sandra saw me several times and never had a hair out of place. She was usually dressed in a skirt and matching jacket with a blouse and court-style shoes. Of course, the conversation was had over footwear, but it was clear that her preferences were strong and would not move. Ultrasound investigation showed the tendon was involved with the lesion compressing down on the sheath of EHL. The epidermo-dermal junction was damaged and the fluid seepage confirmed the chronicity.
Podiatric surgery
One of the approaches a few podiatric surgeons had been using for a few years was the use of the Schrudde flap. This was where a pedicle of skin was created to cover a full-depth defect following excision down and through the adipose layer. The new skin, unaffected by pressure, is complete with a new fat pad and has an extant blood supply from the intact skin pedicle. The procedure was performed in an orthopaedic standard theatre under general anaesthetic. An ankle block was provided before surgery for pain relief upon recovery and to lessen the depth of anaesthesia required. No anaesthetic was infiltrated near the skin flap. A thigh cuff provided haemostasis and was released before dressing the wound. This ensured good flap perfusion.
The flap, skin and tendon
In this particular case, I utilised a larger pedicle rather than a circular one typical of Schrudde. You could liken this to an inner tube cycle puncture repair. The tissue is removed as a rectangular block and in the case of Miriam, her tendon being damaged was excised and the tendon repaired. The tendon could have been lengthened as a slide but this would not allow the damage to repair effectively. To excise and join the tendon by anastomosis repair would create further tightness and contradict the objective of surgery. A graft could have been used. This would have added to the surgical cost of the procedure and other complications. The tendon was left with a gap, and sutures were crafted to allow the ingrowth of the tendon along the suture lines. The skin was folded over the full-thickness defect so the tendon and defect were covered. Deep and skin closure was affected, the skin with 4/0 prolene. The follow-up period was standard (7 days, 14 days) after a regular dressing and post-operative shoe.
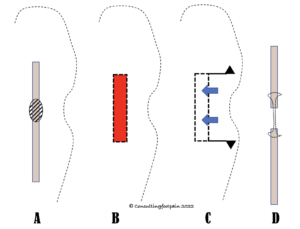
A – extensor tendon showed with the lesion on top. B – the area in red represents full-thickness tissue excised. C – the flap is square with triangular pieces removed. The skin is undermined and translated forwards, allowing the skin to stretch without vascular compromise. D – shows the tendon lengthened and repaired with Kessler style suture method
Suturing tendons the size of the EHL is considerably more challenging than the larger tendons of the foot. A minor setback occurred with deeper (Vicryl 4/0) sutures, one of which came to the surface and was removed under local anaesthetic, providing rapid healing thereafter.
Despite a minor setback, the flap was fully viable





Figures 1-4: (1) the wound is healing after removing a lone suture causing problems. (2 & 3) illustrate healing with minimal graft edges visible and good bedding down the skin. The redness will ebb with time. (4) shows the toe fully extended with a good return of motor power. The humping is due to residual swelling continuing the reparative stage of the deeper tissues and occurs well behind the tendon gap (see video below).
Video of Sandra following full recovery

Histopathology
The standard hospital reports break down into clinical details, microscopy, and a diagnosis (conclusion).
Clinical details: rectangular skin, full thickness, traumatic features, scar tissue, adipose appears poor as does extensor tendon.
Macroscopy: skin 13x8x3mm deep bearing an indurated lesion 5mm.
Microscopy: There is a cup-shaped pit containing a plug of parakeratin and a loss of the granular layer. Deep to this, the dermis is scarred. No foreign body is seen and there is no infection or atypia. The excision of the lesion is close at the deep margin but is well clear peripherally. The appearances are similar to a clavus/corn but are secondary to trauma.
Summary and reflection
Histopathology is valuable for understanding the type of tissues and cells involved in the pathology. The trauma origins can be seen from damage to the skin and tendon. The dermis is affected, meaning conservative care is unlikely to have been successful. This is the case because the extensor tendon has adapted for so long. Exclusion of atypia is important as this rules out cancer but we see no macrophages, common to some keratoma problems, suggesting active infection and inflammation. Confirmation of corn (clavus) is useful despite being obvious to podiatrists.
We must always reflect upon any problems, our decision, the effectiveness of the treatment and whether we could have done anything differently. Patient counselling is always essential and the rationale for conservative treatment should be emphasised along with the patient’s preferences. All intractable lesions can be helped by podiatry, but the EDJ damage and underlying deeper tissues may not respond or may take longer than a patient is willing to persevere. This should be clearly documented, and a follow-up summary should be shared with the patient and GP to include recommendations.
Non-surgical intervention is always better, and such surgery risks include necrosis or failure of the flap. Loss of tendon power. Post-surgical infection and rejection of sutures. Reoccurrence of the lesion is entirely possible if the patient does not observe shoe design recommendations.
In this case, a 73-year-old healthy female had a reconstruction of tendon and skin will a fully functional recovery and was satisfied with her treatment.
 Reference to Image
Reference to Image
Heo, Youn-Moo & Roh, Jae-Young & Kim, Sang-Bum & Kim, Jae-Young & Lee, Jung-Bum & Kim, Kwang. (2010). Contracture of Extensor Hallucis Longus Tendon Occurring after Intramedullary Nailing for a Tibial Fracture. Journal of the Korean Orthopaedic Association. 45. 399. 10.4055/jkoa.2010.45.5.399.
Thanks for reading ‘Obstinate Corns over Tendons’ by David R Tollafield
David is a retired podiatric surgeon and the author of ConsultingFootPain. You can read a wide range of articles on this site. Look out for more articles on corns and callus. You can read the author’s classification system for plantar callus, published by JFAR Journal Publications for David Tollafield
This article was submitted for first publication 10 October 2022
![]()
Published by Busypencilcase Communications Est. 2015
Recent Comments