Clinical Articles

Obstinate Corns over Tendons
We must always reflect upon any problems, our decision, the effectiveness of the treatment and whether we could have done anything differently. Patient counselling is always essential and the rationale for conservative treatment should be emphasised along with the patient’s preferences. All intractable lesions can be helped by podiatry, but the EDJ damage and underlying deeper tissues may not respond or may take longer than a patient is willing to persevere. This should be clearly documented, and a follow-up summary should be shared with the patient and GP to include recommendations.
Research Papers Made Simple
Here are some of the questions worth addressing –
Ask yourself what you need from a paper. Do you need data – numbers, do you need methods, do you need outcomes showing the effectiveness of a method? How up-to-date should the paper be? Is there a limited number of papers on the subject you want to read, or are there dozens of papers? What does the study tell us? What is the outcome? What have I learned and is the paper a good paper? Is there a better paper and can I use this reliably?
Journals are a Marmite thing!
Podiatry Now was unsaddled with the need for higher end academic articles but still produced articles with academic rigour and introduced tougher admission criteria along the lines of an academic design.
Journal of Foot and Ankle Research (JFAR) was launched in July 2008 as the official research publication of the Society of Chiropodists and Podiatrists (UK) and the Australasian Podiatry Council, replacing both the British Journal of Podiatry and the Australasian Journal of Podiatric Medicine. Many changes. Decisions have been made to professionalise the journal for better impact factor, to improve quality and offer better peer review, while retaining a membership publication

Writing for ConsultingFootPain
When asked to write for ConsultingFootPain (CFP), I am asked by many how long should an article should be, what format and when it should be sent in – the deadline. These are all easy questions to answer, but it is worth putting more detail together if you want to write for ConsultingFootPain.
This article is a quick read – under 1000 words which is around a 4-minute read. Reading times
Core Podiatry has Changed
When at college in the mid-seventies there was a general understanding that we all were expected to provide a ‘full-treatment’ – FTx. First of all the FTx implied managing nails and hard skin, apply a cornucopia of padding, whichever fitted best to the needs of the patient and the properties of foam, felt, fleece or foam-o-felt. Appliances (not orthoses in the seventies) became the pinnacle of our prescribing and manufacturing skills. Biomechanics was not a term known to most British podiatrists. Local anaesthetics were in their infancy.
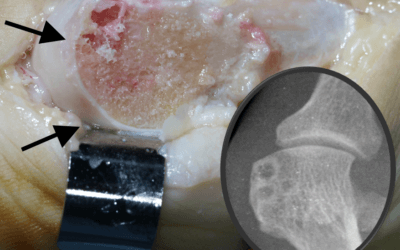
Cartilage Damage in Hallux Valgus
While the observation of cartilage damage often confounds clinicians on how patients manage such extensive cartilage damage this paper visits the real reason behind joint pain.
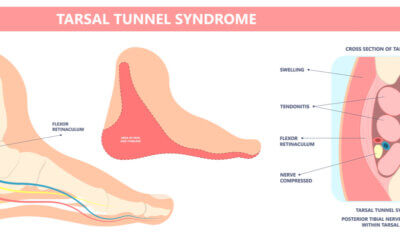
Tarsal Tunnel Pain
I want to introduce you to the condition called tarsal tunnel syndrome as a cause of heel pain but with the distinctive quality that the pain burns. The second feature that gives the condition away is that feeling of fullness, a sort of exploding sensation when exercising worsening with standing walking or running. Sometimes this type of problem pain is called referred. This means that the source of pain and location may not match. The pain may be in front of the foot but is related to the structures in the hind part of the foot.

More About Heel Problems
The most common types of heel pain problems arise from general overuse or repetitive heel pad strain but heel pain is complex and if left can resist treatment. In this article, there are four key subjects that you need to know about. The first relates to children while the other conditions are adult related. There are conditions such as rheumatoid arthritis, gout and ankylosing spondylitis that may affect the heel as well as rarer conditions and of course fractures. If the pain does not subside with self-help remedies recommended after several weeks, then seek professional medical help from a podiatrist or medical practitioner.

Biomechanics and the foot orthosis
In the USA, from the sixties, the earlier designs were based around a popular subject called ‘biomechanics’. This was a pseudo term but became a significant part of the podiatric medicine degree course in the USA. Much of this pseudo-science involved measurements with protractors (tractographs) and in build error ‘eyesight’ assessment which led to assumptions with a predilection for the concept of wedging. The foot orthosis (F.O.), as it was called, tried to separate itself from the older insole and appliance. A google search today will still confuse the terms.
First Use of Corticosteroids by UK Podiatrists
There has been no previous podiatric publication regarding the use of local corticosteroids in the UK; indeed, in the USA podiatric literature studies have often been conducted empirically by retrospective analysis. It was decided to look at the range of foot pathology routinely treated with local corticosteroids to establish the clinical effectiveness of two preparations. Local glucocorticoid action is a common method used to treat inflammatory pain and one that is well recognized in clinical practice the world over.