Ankle Sprains and Strains
In this article, I focus on why ankle sprains or strains occur. First aid requirements and treatment strategies can be found in treating ankle sprains. This is part of a series of ANKLE articles for ConsultingFootpain. Why not read my articles and series about the ankle joint? You can go to my content page. For more information about sprains, I would recommend one of my favourite education sites, FootEducation. I will say more about this later.
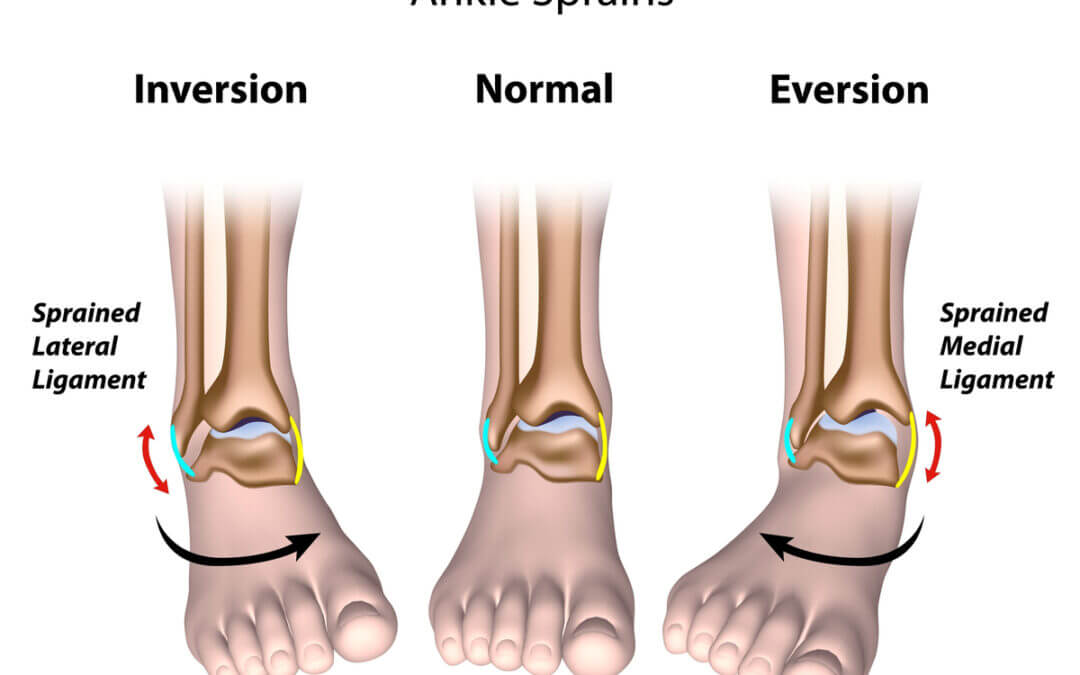
The ankle is complex but is not just made up of one but three major joints. This allows the foot to cope with different terrain (picture author on a typical uneven surface—pebbles) when the hind foot ankle components are working normally. The feature picture shows ankle movements in two directions. It is the lateral ankle strain that is most common, as the ligaments are weakest on the outside and strongest on the inside.

What is an ankle sprain?
The Ligaments
Why does the foot go over?
What if it is not a simple ankle sprain?
What is an ankle sprain?
It is unlikely that you will not have heard about ankle sprains. They can be disabling, cause limping and prevent exercise. The foot swells, including making the ankle larger. A sprain is where a forced stretch overrides the normal control mechanism. This can occur on flat and uneven ground. When on flat ground, this comes as a shock, but it relates to the way we place our feet down. Sprain is the condition, while strain is related to the mechanics of the injury. If we strain any material, it will stretch according to its elasticity until it breaks.
The ligaments of the ankle
Let’s take a look at the ankle ligaments concerned. There are three ligaments. Each is made up of tough parallel protein fibres called collagen. These are shown. The calcaneo-fibular ligament (CFL) and anterior talo-fibular ligament (ATFL) shown are commonly implicated.
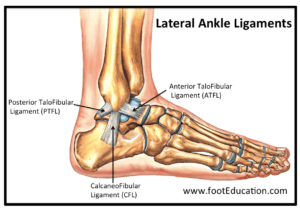
Outside (lateral) ligaments of ankle c/o FootEducation 2020
The mechanism of injury
The ligament is stretched as the ankle ‘goes over’. The ‘going over’ is referred to as the tipping of the outside of the foot. This occurs in almost any activity. Normally, we overcome this quickly as we have special sensors to correct the overbalanced position. The ankle swells and causes us to limp when the ligament is pulled. The limp may last minutes or remain for weeks. Damage to an ankle can develop into a longer-standing problem if ignored. More detailed ankle conditions can be found using the link below. While most ankles settle with this type of simple strain, deeper tissue damage may leave lasting problems. Bruising may appear alarming but will settle sometimes after several weeks.
We must be clear. If ankle pain does not settle, seek professional help. To show just how complex ankle pain is, you can go to this valuable FOOT SITE: https://footeducation.com/foot-pain-identifier/. The FootEducation site is more detailed and has a video by Kenneth Hunt (2.36 min).
Why does a foot go over?
Movement in the ankle is most vulnerable when going downhill. You can read more about this in my earlier article on the true ankle, The Ankle, and its role in walking. Bound by strong ligaments on the inner side (not shown) and weaker ligaments on the outer side, shown in the featured image, the movement we call inversion is much greater than eversion. The subtalar joint below the ankle joint provides side-to-side movement, inversion and eversion. The range of Inversion is 3-4 times more than eversion usually.
Many would consider this an immediate flaw in the human frame, but without the inversion movement, we would not cope with uneven ground as we do. It is, therefore, a question of compromise. Suppose we go downhill, and the ankle tips toe down, using the narrow part of its curved surface. The moment this happens the ankle is less stable. If we go uphill, the ankle uses the broader part of the curved surface and is more stable. Eversion movement at the subtalar joint is more stable and supported by stronger inner ligaments and tendons. Most ankle sprains occur when the ankle is toe down and maximally inverted at the subtalar joint.
Boots with higher rear support are recommended because of inversion instability on rigged terrain. The boot adds ankle support and stability. Boots will not prevent sprains, but they will minimise the extent of injury. Kenneth Hunt, in his video, describes the stages of ligament injury, from simple sprain to rupture. In the diagram below, the illustration suggests different effects of one or more of the ligaments.
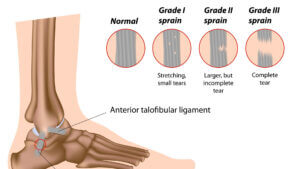
Alila medical media/Shutterstock.com This is illustrative only and is intended to provide a lay guide. It should not be taken to mean a specific grading system used in medicine.
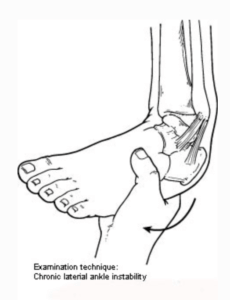
Inversion was demonstrated to highlight ankle instability. This is not reliable. Special investigations are required because of ‘guarding’. The picture was taken from Foot Health Facts American College of Foot & Ankle Surgeons. Accessed 4/12/20
The most curious aspect of ankle sprains is that we cannot always predict if or when they will happen. Some factors that we know will increase the likelihood of sprains are previous known injuries, which make a difference to the chances of repeating damage, and certain foot types that increase the tipping over of the foot, e.g., high-arch feet. High-risk sports will expose the ankle to damage to a higher grade range.
Weak ligaments as a cause
In this case, the ankle’s anatomy implies that it has more movement than it should. When exposed to the plantar flexed-inverted position, the joint opens more than it should.
- “As early as the 1950s joint ligaments were demonstrated to contain sensory endings that are sensitive to small changes in ligament tension and to passive joint movements.” Sjölander P., Johansson H. (1997)
If we put this in context, we find the word proprioception or knowledge of the position of a joint. Information is transmitted to the brain by sensory nerves called proprioceptors so adjustments can be made. Any change in the position of the ankle is regulated up to a point. The messages and signals may well be interrupted by other factors, causing us to lose balance and hence injure the ankle momentarily. The possible cause of chronic ankle instability is a combination of diminished proprioception and muscle weakness known as the ‘evertors’ of the ankle. This being the case, Willems T, (2002) recommended proprioception and strength training in the rehabilitation program for ankle instability. This is explained below.
Take a simple example. You are balanced on the edge of a swimming pool. It is known that a point arises that if you fall forward, a point will have been reached where you cannot correct your fall. Muscles will work to make posture corrections up to a point until the muscles cannot assist further. The ankle evertors, for instance, prevent inversion. Inversion is the major cause of sprains because the ligaments cannot cope with overbalancing. Foot and ankle specialists will not just look at the ligaments but also the muscle tendons on the outside of the ankle for damage. If we are to help, we can apply first aid but must also take steps to prevent the ankle from re-injuring.
Not an ankle sprain?
Unfortunately, due to the mechanics of some injuries, such as sports injuries, car accidents, falling off ladders at home, or simply slipping on leaves on a path, ankle conditions are not always limited to simple sprains. Use this simple guide.
If your pain and swelling have not improved and all the advice given is making matters worse, you may not have a sprain. Seek help because the problem may need a different solution, and these are outside first aid. These are listed below but are technically more complex to understand. This list is provided to demonstrate other problems that can confuse people as to the reason for their slow recovery from an ankle sprain.
Alternative concerns
- Peroneal tendons split tear (evertor tendon)
- Chip fracture off fibula bone
- Inflammation in deeper groove (sinus tarsi)
- Tear of shorter peroneal tendon and styloid process
- Dislocating tear damaging outer ankle joint
- Non-displaced fracture of the fibula
- Joint lining (synovitis) chronic inflammation
- Cartilage defect
- Ganglion pain
- Ankle joint infection
- Loss of blood to the main ankle bone (talus) called necrosis
Each of these conditions can manifest in chronic problems which never improve. The details for understanding will fall under the Clinician Portal or can be found under FootEducation.com

Sjölander P., Johansson H. (1997) Sensory Endings in Ligaments: Response Properties and Effects on Proprioception and Motor Control. In: Yahia L. (eds) Ligaments and Ligamentoplasties. Springer, Berlin, Heidelberg. https://doi.org/10.1007/978-3-642-60428-7_
Willems T, Witvrouw E, Verstuyft J, Vaes P, De Clercq D. Proprioception and Muscle Strength in Subjects With a History of Ankle Sprains and Chronic Instability. J Athl Train. 2002;37(4):487-493.
Thank you for reading my ANKLE SERIES and, in particular, ‘Ankle Sprains and Strains’
by David R Tollafield
![]()
Published by Busypencilcase Reflective Communications Est 2015
Released 27 December 2020. Modified January 2025.
![]()
Recent Comments