
Professional Clinical Resources
Independent prescribing and continuous professional development for podiatrists
 Professional clinical resources are vital for the demands imposed on all clinical practitioners. Several authors in podiatry have authored professional materials referred to as ‘pullouts’ delivered through journal magazines and webinars. This article and clinical resources follow the backdrop of independent prescribing recently covered within podiatric circles. Dr Tim Kilmartin (pictured) has been a strong proponent. The only problem with published articles is that access to the information can be lost unless accessible through formal publications or electronic access. His articles are detailed learning sheets that have immense value, not least because they are free. The importance behind many of these articles is that the person providing the information is highly knowledgeable in podiatric medicine. Tim Kilmartin is well known for his exceptional publishing record.
Professional clinical resources are vital for the demands imposed on all clinical practitioners. Several authors in podiatry have authored professional materials referred to as ‘pullouts’ delivered through journal magazines and webinars. This article and clinical resources follow the backdrop of independent prescribing recently covered within podiatric circles. Dr Tim Kilmartin (pictured) has been a strong proponent. The only problem with published articles is that access to the information can be lost unless accessible through formal publications or electronic access. His articles are detailed learning sheets that have immense value, not least because they are free. The importance behind many of these articles is that the person providing the information is highly knowledgeable in podiatric medicine. Tim Kilmartin is well known for his exceptional publishing record.
As a consultant and former full-time lecturer (Northampton & Belfast), he has provided podiatrists with placements and fellowship programmes. These CPD documents highlight the attitude of sharing our knowledge and expertise with a wider community.

I would commend members to Tim’s latest article in the series Clinical Emergencies now published in ‘The Podiatrist’ for members of the Royal College of Podiatry released March-April 2021. The series, advertised, supports independent prescribing, which I have briefly covered elsewhere. The subject represents a significant change to all podiatric practices. The subtext for each of these articles is mixed with my own commentary below as a brief abstract. I have, as usual, used hyperlinks to offer more information about the subject. The additional value will appeal to students and post-graduates studying at the MSc level and for their Independent Prescribing course qualifications (Editor).
Dr Tim Kilmartin FCPodS, PhD, reflects how the idea of CPD pull-outs started for him…
The Ethos behind Tim’s professional articles
“Back in the early ’80s, Pete Boden and a few others from Manchester foot hospital wrote a series of articles for ‘The Chiropodist’ on Biomechanics. They did forefoot varus one month, then rearfoot varus the next etc. I thought they were groundbreaking as I was a student struggling with biomechanics at the time. I wrote those CPD articles in the same vein, i.e. we are on the brink of massive practice change with independent prescribing everyone needs to have it pointed out to them. I thought they would be particularly invaluable to those doing the MSc in podiatric surgery as I reckoned they would cover the entire course! In fact, I don’t think many people even noticed them, so to have them not forgotten is most encouraging…” Tim Kilmartin 2021
Reflecting on professional development changes
These articles are only available for members of the Royal College of Podiatry who subscribe to the journal in the past. Please contact the Royal College of Podiatry for back articles.
- Analgesics – Podiatry Now 2018. 21 (1): 1-11
- Antibiotics – Podiatry Now 2017. 20 (5): 1-11
- The Management of Osteomyelitis – Podiatry Now. 2016 19 (5): 1-10
- Deep venous thrombosis management – Podiatry Now 2016. 19 (11):1-1
‘Podiatry Now’ was the former journal issued monthly for the College of Podiatry. In January/February, the replacement bi-monthly journal ‘The Podiatrist’ was issued in 2021 in association with the newly appointed Royal College of Podiatry.
Analgesics for Podiatrists and Independent Prescribers
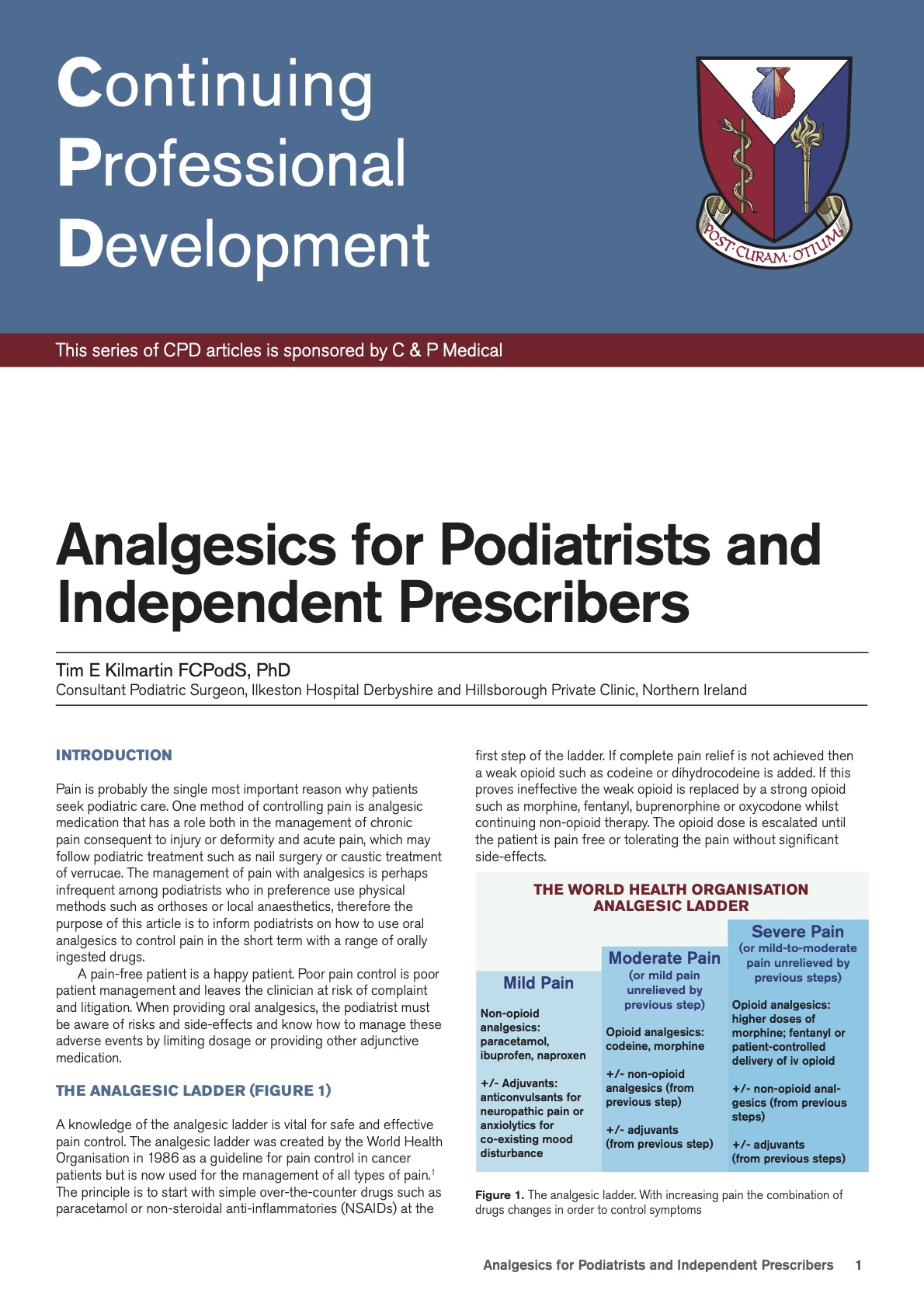 The management of pain with analgesics might be infrequent among podiatrists. Indeed in my own articles on pain management for patients, much can be gained from OTC products. We now learn through Covid more than before that all medication cannot be assumed to suit one group in the population. This has focused on gender, but it is only time when racial discrepancies will pick up greater attention to what drug is best. Tailoring drugs will complicate the education of prescribing patterns. For the moment, we are left with a broader application but one that must take us away from the OTC medication. Tim’s article informs podiatrists how to use oral analgesics to control pain with a range of orally ingested drugs. A pain-free patient is a happy patient but intended only for short term use. Poor pain control is poor patient management and leaves the clinician at risk of the complaint. However, the podiatrist must be aware of risks and side effects and know how to manage these adverse events by limiting dosage or providing other adjunctive medication.
The management of pain with analgesics might be infrequent among podiatrists. Indeed in my own articles on pain management for patients, much can be gained from OTC products. We now learn through Covid more than before that all medication cannot be assumed to suit one group in the population. This has focused on gender, but it is only time when racial discrepancies will pick up greater attention to what drug is best. Tailoring drugs will complicate the education of prescribing patterns. For the moment, we are left with a broader application but one that must take us away from the OTC medication. Tim’s article informs podiatrists how to use oral analgesics to control pain with a range of orally ingested drugs. A pain-free patient is a happy patient but intended only for short term use. Poor pain control is poor patient management and leaves the clinician at risk of the complaint. However, the podiatrist must be aware of risks and side effects and know how to manage these adverse events by limiting dosage or providing other adjunctive medication.
All podiatrists qualifying since 2008 with a prescription-only medicines – sale/supply certificate can supply and issue the following oral analgesics: ibuprofen, codeine phosphate 30mg, co-codamol (8/500) and co-dyramol. These medications are effective for mild to moderate pain. Supplementary and independent prescribers can prescribe more extensively, allowing management of more severe pain. The formulary available to podiatric independent prescribers includes NSAIDs, ranging from naproxen to indomethacin and non-opioid analgesics including nefopam, gabapentin and pregabalin.
Independent prescribing and antibiotic prophylaxis in podiatry
 There has been much talked about prophylaxis not helped by the mixed views about resistance and overuse of antibiotics in medical practice. This article might appeal more to podiatric surgeons and extended scope podiatrists as high-risk foot specialists. The value behind this professional clinical resource should be considered as background justification for prophylaxis and applies to less complex procedures such as onychocryptosis. antibiotics
There has been much talked about prophylaxis not helped by the mixed views about resistance and overuse of antibiotics in medical practice. This article might appeal more to podiatric surgeons and extended scope podiatrists as high-risk foot specialists. The value behind this professional clinical resource should be considered as background justification for prophylaxis and applies to less complex procedures such as onychocryptosis. antibiotics
Independent prescribing allows podiatrists to manage a range of pharmaco- logically as a more direct and timely approach. It also allows podiatrists to use medicines to prophylaxis against significant treatment-related issues such as anxiety, venous thromboembolism and post-operative wound infection. In this article, the evidence base for antibiotic prophylaxis in podiatry is considered. Though the main indication for antibiotic prophylaxis is in podiatric surgery, all podiatrists performing invasive procedures must be aware of the risk factors and indications for antibiotic prophylaxis.
The value of providing antibiotic prophylaxis to reduce the risk of post-operative wound infection following skin, nail or bone surgery is a contentious issue. After much discussion within the profession, it still proves difficult to reach a consensus. The evidence base for every aspect of antibiotic prophylaxis is extensive though very little refers specifically to the foot or podiatric practice.
Independent Prescribing and the Management of Osteomyelitis
 Having read correspondence from podiatrists in a string of Facebook comments, the knowledge in general practice around osteomyelitis is patchy. The lack of confidence in approaching osteomyelitis is transparent, and yet with more knowledge, the baseline outcome would allow better referrals where the invasive scope is not possible. The basis of management is diagnosis, confirmation and action. The use of drugs to deal with osteomyelitis is important, and Tim Kilmartin’s CPD article seeks to provide a clinical approach to the management of osteomyelitis.
Having read correspondence from podiatrists in a string of Facebook comments, the knowledge in general practice around osteomyelitis is patchy. The lack of confidence in approaching osteomyelitis is transparent, and yet with more knowledge, the baseline outcome would allow better referrals where the invasive scope is not possible. The basis of management is diagnosis, confirmation and action. The use of drugs to deal with osteomyelitis is important, and Tim Kilmartin’s CPD article seeks to provide a clinical approach to the management of osteomyelitis.
Although it is a podiatric surgery case, it is hoped that the treatment plan described could also be applied by Podiatrists involved in diabetic foot care who will consider independent prescribing as a natural progression in their professional development, enhancing their role as the diabetic foot specialist and allowing them to manage the at-risk diabetic foot comprehensively. How this case was managed would not have been possible before independent prescribing. The patient would have been referred to another speciality and more than likely lost to follow up with the possible consequence of litigation.
Before independent prescribing, the list of drugs available to Podiatrists was limited and insufficient to manage all aspects of podiatric care. With GP appointments and skills sets altered by the corona viral storm, podiatrists must start to drift away from their comfort zone and become more proactive. If you suspect a problem, then professional management starts with your practice.
Preventing Venous Thromboembolism and Independent Prescribing
 They often say that blood clots are silent killers, and it is for a good reason. It is no accident that thrombotic disease required podiatric surgeons to understand once patients were exposed to periods of immobility. There are no apologies that Tim Kilmartin uses surgery as a backdrop to advocate podiatrists must assume better knowledge. The first pertinent point to make is that we are lower limb specialists. The second point to mention is that podiatrists are often first responders. To miss an obvious deep vein thrombosis is less acceptable today than it might have been in general practice.
They often say that blood clots are silent killers, and it is for a good reason. It is no accident that thrombotic disease required podiatric surgeons to understand once patients were exposed to periods of immobility. There are no apologies that Tim Kilmartin uses surgery as a backdrop to advocate podiatrists must assume better knowledge. The first pertinent point to make is that we are lower limb specialists. The second point to mention is that podiatrists are often first responders. To miss an obvious deep vein thrombosis is less acceptable today than it might have been in general practice.
The purpose of this article is to alert all podiatrists to the significance of venous thromboembolism (VTE) and its potential for complicating the recovery of any podiatric patient who is immobilised following injury or treatment. It is also an opportunity to highlight the emerging role of podiatrists as independent prescribers who can now access medicines to prevent and treat this condition. The management of patients already taking anti-coagulant or anti-platelet therapy is also considered in the context of invasive procedures such as nail, skin or bone surgery.
A case study is used to consider the medicines management of a patient at risk of developing a VTE following podiatric surgery and select the appropriate therapy which could reduce the potential mortality and morbidity associated with the condition. The management of the patient is conducted based on the National Institute for Health and Care Excellence (NICE) guidelines.
Editorial Comment
The above CPD papers are three years old, or more, and were published in ‘Podiatry Now’ We approached the Royal College of Podiatry to promote these resources and Emma Godfrey, their Editor advised; “The CPD pieces are College material and permission to reproduce or run anything elsewhere is not granted on all occasions.” Naturally, ConsultingFootPain is disappointed that such eminent material will not be made available after all the hard work that the author has put in for members. It is very much hoped that those who can consider publishing all the older CPD pullouts easily to reach place for members will do so.
Policy statement
ConsultingFootPain (CFP) made a decision in 2020 to turn all previous publications under Reflective Podiatric Practice for Open Review. Those not currently accessible will be published in due course. It is understandable that journals wish to preserve materials for their members as a privilege, but Busypencilcase Communications believes these trends are changing. Any author, layperson or professional can write for CFP free. We are unable to pay authors but support those who wish to learn the craft of writing. We do not accept student’s formal coursework before completion of university studies.
Thank you for reading Professional Clinical Resources by David R Tollafield
Published July 2021 by Busypencilcase Reflective Communications Est.2015
![]()
Recent Comments