A Guide to a Career in Podiatric Medicine
Launching A New Career Book Looking back seems like a lot of water under the proverbial bridge. It started as an invitation from two schools to speak to their 8-10-year-olds and 11-15 years olds in April 2019. 'Inspiring the Future is a charity promoting careers to...

Thoughts on the Hammer Toe
When the foot flattens or heightens, the muscles’ position and tendons change, exerting a different pull. This concept has been in vogue since the sixties emanating from US podiatry education and scholastic theory.
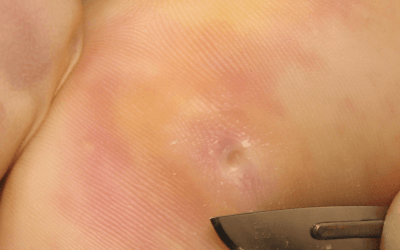
Treating Corns on Feet
In Part 1 – The corn is part of the keratin layer and does not penetrate the basement membrane because the area would bleed if it did. There are other reasons the dermis is penetrated, not least due to penetrating splinters. However, in some cases, infections and changes arise where blood vessels become invested between the dermis and epidermis, as seen in wart infections (a virus). These have been erroneously called vascular corns or neuro-vascular corns.

Where does patient blockage lie?
The same recruitment issues exist in the NHS and the private sector. On top of this, the fabric of healthcare is under greater strain because people have been neglecting their feet a lot more than they did before, and problems have built up over those two years where they weren’t doing things. So people having foot health checks every four to six months haven’t had them for two years, and small problems became big problems, and therefore needed more treatment.
At the same time, people are more health aware, more fitness aware, and more on their feet, so it’s a combination of more patients wanting podiatry with less availability. So we have a trio of factors: funding essentially, patients failing to check their feet, so the problems have built up during the Covid period, and lastly, better health awareness is actually drawing them out of the public arena now.
Should you befriend patients?
It is likely that podiatrists or others reading this article, feel it is essential to bond, and create a sense of trust through light-hearted banter. Perhaps we think we are better liked and can outclass an old practitioner who hardly breaks a smile. It would be unusual for any self-respective clinician to be unaware of the subject of body language but the non-verbal cues are essential. A smile never hurts, but it is listening that is vital.

Obstinate Corns over Tendons
We must always reflect upon any problems, our decision, the effectiveness of the treatment and whether we could have done anything differently. Patient counselling is always essential and the rationale for conservative treatment should be emphasised along with the patient’s preferences. All intractable lesions can be helped by podiatry, but the EDJ damage and underlying deeper tissues may not respond or may take longer than a patient is willing to persevere. This should be clearly documented, and a follow-up summary should be shared with the patient and GP to include recommendations.
Research Papers Made Simple
Here are some of the questions worth addressing –
Ask yourself what you need from a paper. Do you need data – numbers, do you need methods, do you need outcomes showing the effectiveness of a method? How up-to-date should the paper be? Is there a limited number of papers on the subject you want to read, or are there dozens of papers? What does the study tell us? What is the outcome? What have I learned and is the paper a good paper? Is there a better paper and can I use this reliably?
Journals are a Marmite thing!
Podiatry Now was unsaddled with the need for higher end academic articles but still produced articles with academic rigour and introduced tougher admission criteria along the lines of an academic design.
Journal of Foot and Ankle Research (JFAR) was launched in July 2008 as the official research publication of the Society of Chiropodists and Podiatrists (UK) and the Australasian Podiatry Council, replacing both the British Journal of Podiatry and the Australasian Journal of Podiatric Medicine. Many changes. Decisions have been made to professionalise the journal for better impact factor, to improve quality and offer better peer review, while retaining a membership publication

Writing for ConsultingFootPain
When asked to write for ConsultingFootPain (CFP), I am asked by many how long should an article should be, what format and when it should be sent in – the deadline. These are all easy questions to answer, but it is worth putting more detail together if you want to write for ConsultingFootPain.
This article is a quick read – under 1000 words which is around a 4-minute read. Reading times
Core Podiatry has Changed
When at college in the mid-seventies there was a general understanding that we all were expected to provide a ‘full-treatment’ – FTx. First of all the FTx implied managing nails and hard skin, apply a cornucopia of padding, whichever fitted best to the needs of the patient and the properties of foam, felt, fleece or foam-o-felt. Appliances (not orthoses in the seventies) became the pinnacle of our prescribing and manufacturing skills. Biomechanics was not a term known to most British podiatrists. Local anaesthetics were in their infancy.