Clinical Articles

A Bone Swelling on the Big Toe
An injury to the toe is common, not least because the toe sticks out at the end of the body. The excessive growth, like hyper granulation in an ingrown toenail, confuses the clinician because the skin is shiny, stretched, red and easily knocked. I always sent off my bone samples once removed at our local hospital for some years, and they used a specialist hospital in Glasgow to peer review any interpretation. I knew that elsewhere in the body, the bone-cartilage lesion known as an osteochondroma could become malignant in <5% of cases, but in the foot, this is rare.
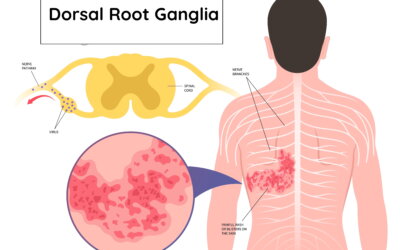
Pain and the Dorsal Root Ganglia
The long-term effect of the nerves within the DRG failing to settle after being affected causes skin blisters at the end of those nerves where the DRG becomes active. As the blisters either burst or crust over, the itching and burning sensation settles slowly but still leaves a sensitivity. If the sensitivity continues, despite the skin rash and blisters no longer being visible, the condition becomes both chronic and complex.
Podiatry Business From Scratch
Whether you are starting your business following graduation or transitioning within the podiatry sector, there are several red flags to watch for. We should refer to them as green flags to counter any notion that independent practice is something to be avoided. This article looks at clinical practice from a static base rather than a domiciliary practice, although there are principles that overlap. Naturally, in such a short space, it is not possible to cover every aspect. More resources can be found at the end.

The Physician’s Eye
The state of observation can only provide a suspected condition and is far from definitive. A clinical examination requires the patient to provide information, but the clinician will observe and listen to exclude the most obvious signs of disease before taking the all-important history. The chance of cardiovascular disease may well be suspected by facial colour, which includes the lips. The next time you see a doctor or specialist, you will be more aware of the fact that you are on show the moment you enter the room. Like a computer, he or she is processing you, gathering data and may have a diagnosis already!

The Clinical Visit
Comprising three distinctive parts, the clinician uses the five senses to guide the process–one might take the humourous view of Sherlock Holmes or Poirot in determining evidence from visual observation and verbal questioning. I hope these small introductory articles provide some interest. The first in the series covers observation as in the Physician’s Eye.

Why Can’t You Make Ganglions Disappear?
Hitting any tissue is not recommended, and indeed, one should avoid using computer tablets and iPads in place of the Bible – that is, unless you are searching for information such as this site, then hit the keyboard instead.
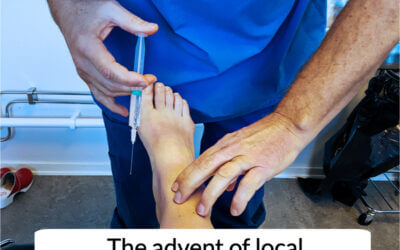
When did podiatrists first use local anaesthetic?
The story of when podiatrists first use local anaesthetic was published here at ConsultingFootPain in August 2018. I have updated this slightly because a recent article in the January 2021 edition of The Podiatrist- ‘rising from the ranks’, has provided a little more information which is worth highlighting (Potter, M). Additionally I go behind the scenes in my latest book, Podiatrist on a Mission.
How Long Does Bunion Surgery Last?
Fusion is a safer bet than most alternatives and offers better longevity. Third surgeries seldom come without loss of function. More surgery involves deeper tissue scarring, and even then, a joint-sparing operation could lead to limited joint movement. Minimal incisional surgery (MIS) appeals to many for obvious reasons, but the follow-up is not as well presented as other surgeries and is limited to specific criteria. MIS is available and has advantages. New screw systems allow surgical placement through keyholes under X-ray-guided control.

Writing From The Past
“At the time [1978] research in chiropody was rather sparse, poorly owing to the lack of a foundation degree. In one paper from a US doctor [DPM], there was extensive material covering bacteria recovered from surgical infections. This left me in awe of their academic standards and only heightened my ambition to become a podiatrist.
Back at Weston Favell clinic, I bumped into April Reilly, the sister who ran the GP’s clinic. ‘I see you’ve got your own autoclave now. You won’t be needing mine anymore is that right? She said in jest.
I just smiled and said, ‘Anyway, not sure if you’ve heard, but Luuk has just promoted me after a year. Not bad eh’ I exuded happiness in sharing my the news.”

Osteomyelitis
Defining a role and executing a treatment plan does not just include performing a physical service. All podiatrists are trained in medical sciences. The principle of what one does is predicated on knowledge, training and exposure. The qualification, without doubt, aids action, but what if you do not have a fellowship? Those podiatrists who deal with lepromatous ulcers and, in particular, neuropathy should and can remove bone if this is observable because they understand tissue compliance.